A 73-year-old man with recurrent squamous cell carcinoma that had spread to his nasal septum, nose bridge, and lymph nodes (stage cT4aN2bM0) had previously undergone a partial rhinectomy and forehead flap reconstruction at another facility. He later had a second partial rhinectomy along with bilateral neck dissection. Pathology revealed advanced disease (pN3b) with extranodal extension (ENE+). Due to scarring from earlier procedures, a tissue expander was placed beneath the skin on the right side of his forehead.
Following radiation therapy with additional adjuvant treatment, his reconstructive surgery was postponed for six months to allow for healing. During this waiting period, his columella (the tissue that separates the nostrils) gradually shifted and began to bend to the left.
The surgical team planned a full nasal skin reconstruction using a forehead flap, which would be connected to the remaining columella using an open rhinoplasty-style incision. The shared goal between the team and the patient was to restore the nose’s appearance as naturally as possible. To achieve this, computer-aided design (CAD) technology was used to ensure precise shaping and measurement.


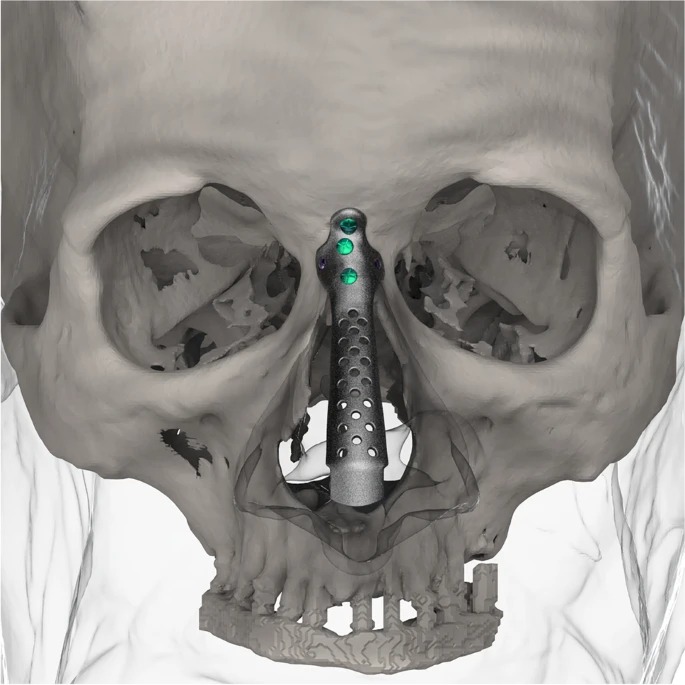
Using ultrasound, the right supratrochlear artery was mapped out, and the forehead flap was designed accordingly. To reconstruct the inner lining of the nose, local hinge flaps from the cheeks were also planned.